
The idea of a health system that provides services and financial protection to all citizens has emerged shortly after the Second World War, through the development of the welfare state. In more recent years, the concept of Universal Health Coverage (UHC) emerged with the World Health Report of 2010 and was endorsed by the UN General Assembly in 2012. Since its inclusion in 2015 in the Sustainable Development Goals, however, UHC has gained unprecedented momentum, as countries around the world have begun defining their own paths towards achieving it by 2030.
In the second part of our series on Universal Health Coverage, we look at how the EU is supporting partner countries to achieve UHC, through mechanisms like the IHP for UHC 2030, the UHC Partnership, and the SPHIP programme.
|
The UHC Day On 12 December, DG DEVCO Deputy Director General, Marjeta Jager and Matthias Reinicke, are attending the high-level UHC Forum in Tokyo, joining hundreds of partners to monitor global progress towards achieving UHC and discuss multiple technical aspects related to future efforts to achieve UHC through multi-stakeholder action, and to learn from country experiences. The opening of the Forum, on 12 December, also coincides with the World UHC Day, celebrated this year for the second time. |
From IHP+ to UHC2030
Since the 2005 Paris Declaration on Aid Effectiveness and the 2011 Busan High Level Forum on Aid Effectiveness, the principles of effective development cooperation (EDC) have been at the core of the development work done by the European Commission’s Directorate-General for International Cooperation and Development (DG DEVCO).
For this reason, when the International Health Partnership (IHP+) was launched in 2007 to promote Health Systems Strengthening (HSS) and effective development cooperation in the field of health, DG DEVCO joined the initiative as one of the steering partners.
To help development partners increase the effectiveness of health aid in partner countries, IHP+ adapted the global EDC principles into the so-called Seven Behaviours, guiding stakeholders towards improved cooperation for HSS.
Bringing these principles into practice, IHP+ has also developed tools to guide sector dialogue and planning at country level, including the Joint Assessment of a National Health Strategy (JANS) and the Joint Annual Health Sector Reviews (JAR).
In 2016, IHP+ began a transition process to expand its scope and mandate. Today IHP+ is known as the IHP for UHC 2030 (UHC2030). The aim of the transition was to better respond to the newly agreed SDGs, defining a way forward for continued support to countries in their HSS efforts, with a view to achieve UHC.
|
Key objectives of the IHP for UHC 2030
For more visit UHC2030’s website |
DG DEVCO has been supporting the transition from IHP+ to UHC2030, and today is still involved in the process, by participating in the UHC2030 Steering Committee, and in two of the organisation’s working groups – the first one to define an approach to HSS and UHC in fragile and challenging operating environments, and the second focusing on sustainability and transition from external financing.
According to Matthias Reinicke, Health Policy Officer at DG DEVCO, the EU has fully supported IHP+’s transformation into UHC2030. “UHC2030 corresponds to the EDC principles laid out in the EU’s Agenda for Change and the Paris Declaration on Aid Effectiveness,” he said. “In particular the principle of ownership – letting the developing countries set their own strategies for poverty reduction, improve their institutions and tackle corruption.”
Co-hosted by WHO and the World Bank, UHC2030 serves as a platform for knowledge sharing, advocacy and coordination for HSS. As a multi-stakeholder initiative, it also helps with monitoring of accountability and progress towards UHC at global and country levels.
|
The UHC 2030 Global Compact
Read the entire Global Compact here |
Since the transition, UHC2030 has expanded its membership, bringing together 60 countries, 11 multilateral agencies and global health initiatives, three philanthropic institutions and five civil society organisations, all of which have signed the UHC2030 Global Compact and committed to working together towards common goals.
In addition, the organisation benefits from the collaboration of a number of highly-specialised initiatives, focusing on strengthening health systems in either specific or comprehensive ways. “The wealth of innovation and knowledge brokered through UHC2030 is unprecedented,” said Reinicke.
The UHC Partnership
In 2011, the European Union took another important step towards the achievement of Universal Health Coverage, joining forces with the World Health Organization (WHO) to create the Universal Health Coverage Partnership (UHC Partnership).
While UHC2030 promotes a shared global vision around UHC, the UHC Partnership serves as its country-level resource. As a thematic fund, it focuses on strengthening the dialogue on national health policies, strategies and plans related to Universal Health Coverage; it involves 28 partner countries around the world, with 17 more having requested to join.
Watch this video for a brief introduction to the UHC Partnership:
The UHC Partnership is led by local actors, with WHO serving as the main convener and broker of the policy dialogue. Additional support is provided by the Health Programme Managers based in EU Delegations who monitor the progress and help address any challenges.
“Essentially, WHO’s role is to provide technical and administrative assistance to governments in the definition of their health policies, strategies and plans,” said Reinicke. “The EU Delegations, meanwhile, focus on mobilising political support, but they also help to monitor progress in identifying what can be improved.”
The UHC Partnership assists countries in defining health policies, strategies and plans that lead to increased coverage of quality health services, financial protection, and health equity.
This is achieved through sector policy dialogue that brings together key national and international stakeholders to agree ways in which national objectives can be achieved. In addition, the UHC Partnership supports countries in building capacity to monitor and evaluate the implementation of those policies, as well as the establishment of sector review mechanisms.
According to Reinicke, the initiative also responds to countries’ demand with regard to the development, implementation and monitoring of national health financing strategies designed to progress towards the achievement of UHC.
“By acting as a facilitator for health sector policy dialogue, WHO leads an effective and coordinated response of development partners around a country roadmap defined at the time when the country joins the UHC Partnership,” Reinicke said.
|
What is the country roadmap? “Once a country gains membership in the UHC Partnership, an inception mission is organised by WHO staff. During this phase, the Ministry of Health (MOH) convenes with WHO support key health stakeholders to align on a country road map with activities which support the current needs of the country in areas linked to policy dialogue on national plans, health financing and/or effective development cooperation. Each year, or as needed (such as when Ebola occurred in West Africa), activities are revised, and updated according to countries’ needs and progress achieved.” For more, see UHC Partnership’s 2016 Annual Report |
Since 2012, the EU has contributed €51 million to the UHC Partnership, with €28 million allocated for its latest phase. Luxembourg joined the Partnership in 2013 with a €10 million contribution, and Ireland joined in 2017, providing an additional €3.2 million. The UHC Partnership is separate from, but complementary to the EU’s bilateral health cooperation in partner countries.
“The UHC Partnership has been an increasing success over the past years, given that it is a challenging initiative,” Reinicke said. “We’re embarking on a completely new concept; the focus is no longer on the vertical component of health systems strengthening, but on a holistic strategy developed to strengthen the ‘One WHO’ approach, and especially WHO’s role at country level.”
In participating countries, Reinicke added, support through the UHC Partnership has fostered policy dialogue on a comprehensive national health policy, resulting in a greater focus towards achieving UHC, according to the country’s own needs, objectives and capacity. “Also, the dialogue itself has become more inclusive, which is important because the continued commitment of all stakeholders is key,” he said. “The UHC Partnership has helped governments to engage both national and international actors in policy dialogue, and improve their alignment with national health planning.”
Crucial to the UHC Partnership is the close collaboration between the EU and WHO. According to Reinicke, assistance from the EU Delegations to partner countries has resulted in significant improvements in monitoring, visibility and the ability of the EU and WHO to address emerging issues in a timely manner.
Watch the following video for more on the EU’s involvement in the UHC Partnership:
Among the success stories, Reinicke pointed to the response to the Ebola outbreak in 2014, where WHO, through the UHC Partnership, played a key role in widening the policy dialogue to include civil society representatives, who helped disprove some of the rumours among the affected communities about how the disease was spread.
“Meanwhile, in countries such as Togo, South Sudan, and Tunisia,” Reinicke added, “the participatory approach of the UHC Partnership has brought together all the stakeholders in both the monitoring and decision‐making of the development of specific policies.”
In Tunisia, for example, the Social Dialogue Programme, which was supported by WHO under the UHC Partnership, has shown how consultations at a grassroots level can help identify key equity issues in the national health system. The grassroots level involvement, Reinicke said, has resulted in a set of crucial policy recommendations, and “has given considerable momentum to the organising committee and a voice to thousands of people in the country”.
SPHIP and SPEED
There is no doubt that effective health policies have to be grounded in sound evidence, locally generated data and a design process that responds to country needs.
In 2015, DG DEVCO launched the Supporting Public Health Institutes Programme (SPHIP), a five-year, multi-country initiative that aims to strengthen public health schools and institutes in partner countries, supporting them in their function of evidence generation, brokering and dissemination for policy-making.
More specifically, SPHIP’s purpose is to enhance expertise, knowledge and resources of institutions in eight countries, and to establish and strengthen their partnerships with similar institutes in other low- and middle-income countries, as well as with European partners. Through this process, the capacity of the health system to provide stewardship is also strengthened.
This is accomplished through the support of EU Delegations, who manage the projects, with technical assistance and institutional strengthening provided by European academic institutions and the SPHIP Support Team based in the Netherlands and Spain.
With a budget of €23 million, the programme runs eight projects in Africa, Asia and the Caribbean. The projects focus on research for policy in relation to the countries’ key goals (UHC), health issues (like non-communicable diseases and maternal and child health) and the strengthening of specific health systems actors (laboratories or district health departments, for example). In addition, the projects include a capacity-building component related to formal in-country education of health professionals.
“Triangular, South-South collaboration and horizontal learning among Southern institutions is a significant added value of this programme,” said Manuel Couffignal, Health Cooperation Officer at DG DEVCO. “Through study visits and regular exchanges of experiences, public health institutes are adopting approaches, methodologies or curriculums used by other institutes, on various subjects.”
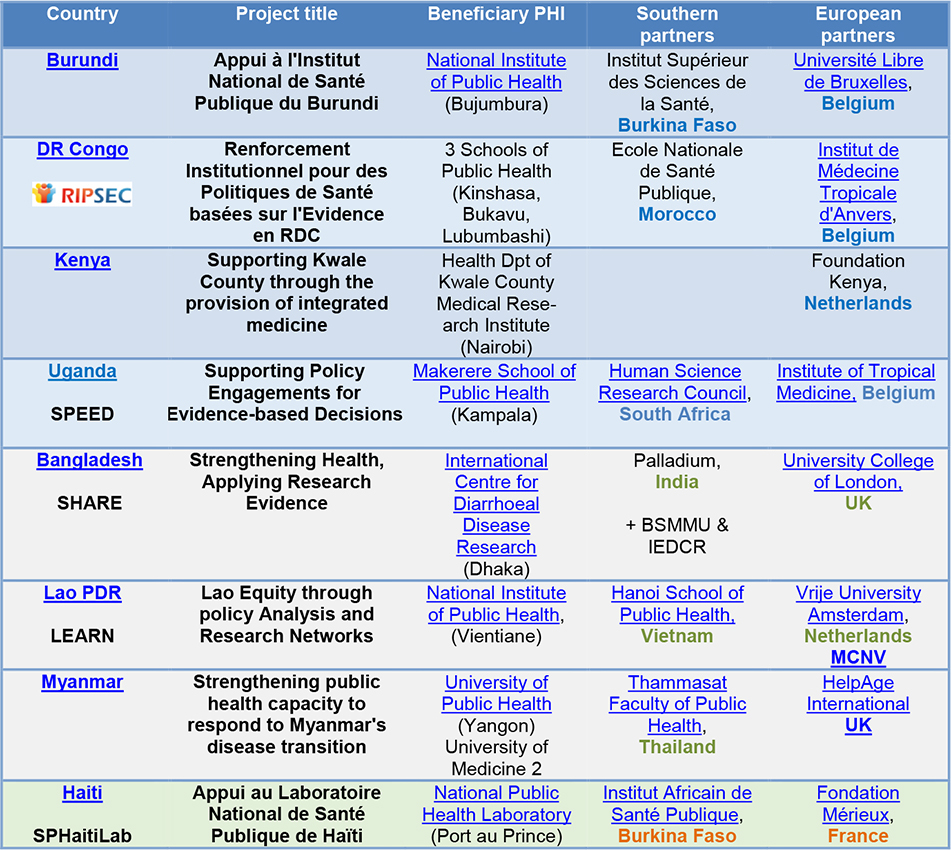
SPHIP projects and partners
One of the projects focusing on UHC is SPEED, or “Supporting Policy Engagement for Evidence-Based Decision Making,” led by the Makerere University School of Public Health in Uganda, in partnership with the Institute of Tropical Medicine of Antwerp, Belgium, and the Human Science Research Council in South Africa. Additional partners in Uganda include the Economic Policy Research Centre, Uganda National Health Consumers’ Organisation and National Planning Authority.
SPEED aims to strengthen Makerere University’s capacity for conducting policy analysis and to build its role as an influential health policy advisor to the government and other partners in the country. While this is happening, the project also addresses some of the country’s key health challenges.
“Uganda has many challenges when it comes to achieving UHC,” said Freddie Sssengooba, the project’s director and associate professor of health policy and systems management at Makerere University. “Firstly, while the government does have some well-developed health policies, it faces substantial challenges in implementing them.”
The other challenge lies in the coordination of all the stakeholders who are supposed to contribute to improving health and well-being of the population. “The Health Ministry is not the only actor working on UHC,” Ssengooba said. “We’ve invited others to work with us, but many of them are not yet aware of what Universal Health Coverage actually entails, or what roles they need to play, individually but also collaboratively.”
Another issue is the capacity for policy analysis. “There is a wealth of research in health science and other areas, but putting this evidence to practical use requires another set of skills,” Ssengooba said, referring to the significant challenges in using evidence for decision- and policy-making processes – one of the key areas of capacity development addressed by the SPHIP. “That being said, we are responsive. The Ugandan government is currently working on health insurance, for instance, and we’re providing them with evidence basis.”
By 2020, when the project finishes, Ssengooba added, “we’ll leave Makerere University with a track record of policy analysis, so it can continue influencing health policy in the country. We’ll also leave behind a set of stakeholders who share a common vision and understanding of what UHC is about.”
For more on what SPEED aims to achieve, watch the following video:
Two years into its implementation, SPEED has managed to gain considerable influence, engaging policy makers with concrete evidence for health policy and systems changes needed to achieve UHC.
“One of our partners has also already come up with the general priorities Uganda should address if it wants to achieve UHC by 2030,” Ssengooba said. “This includes tackling diseases like malaria, which is one of the main causes of morbidity and mortality in Uganda; the issues of reproductive health, particularly contraception; reducing population growth; and reducing the incidence of sexually-transmitted diseases.”
In addition to presenting its research and results at key international public health conferences, the project has also held two symposiums, in 2015 and 2017, that brought together key stakeholders from Uganda and the wider Eastern Africa region to examine how low-and middle-income countries can strengthen their health-financing systems and policies for UHC and health systems development.
“At the last symposium, we had more stakeholders than we could ever envision,” Ssengooba said. “It was a very successful meeting, and it’s still being talked about, both in the media and among the main decision-makers in Uganda.”
According to Couffignal, the European Commission sees compelling value in supporting projects like SPEED. “Health policy development in low income countries is too often dependent on the technical assistance provided by external stakeholders, yet local public health institutes should be best placed to generate the evidence required to inform policies and strategies formulation. Strengthening national ownership and leadership is critical for achieving SDG 3.”
At the moment, Ssengooba and his team are also working on a book that looks back at the health policies implemented in Uganda over the years, to see which of them have worked and why, and which haven’t. “We’re doing this to provide the picture of what’s been happening in the last 10, 20 years, and so we can scale up the practices that actually work,” Ssengooba said. “This will help decision makers to avoid repeating the mistakes of the past.”
This collaborative piece was drafted by the Capacity4dev's Coordination Team, with input from the B4 Unit at DG DEVCO, the coordinators of SPEED and the Health Advisory Service.




(2)
Log in with your EU Login account to post or comment on the platform.
Contratulations for organizing and contributing to the UHC day in Japan and show casing the work of SPEED project in this process.
Greetings to you all.
freddie
Thank you for sharing this post.
Access to Good Health Packages and systems is a universal issue.
If the World Health Organisation, recognises that over 100 million people do not have access to health.
It shows that the SDG Action Goal 3 Good Health and Well-being seems ambitious to achieve by 2030.
The good news is that little changes and EU partnerships, capacity building training has helped countries in developing countries to gain access to local health care services in rural communities and more...
#TogetherGoodHealth
Thank you.